What Is 7-OH? The Emerging Opioid Threat Addiction Professionals Need to Understand in 2026
What Is 7-OH? The Emerging Opioid Threat Addiction Professionals Need to Understand in 2026
By Benjamin Zohar, NCACIP
Nationally Certified Advanced Clinical Intervention Professional
ISSUP New York Network Moderator | NAADAC Professional Member | CCAPP Individual Member
Medical Review: Brandon McNally, RN
Published: March 2026 | Last Updated: July 1, 2026
Table of Contents
- Key Takeaways
- What Is 7-OH?
- Natural Kratom vs. Concentrated 7-OH
- How Potent Is 7-OH?
- How 7-OH Is Sold
- Overdose and Poison Center Concerns
- 7-OH Addiction Risk
- 7-OH Withdrawal
- 2026 DEA and State Legal Update
- Clinical Implications
- Navigating Treatment in New York State
- Related Clinical Resources
- Part of the 7-OH Clinical Education Series
Key Takeaways
- 7-hydroxymitragynine (7-OH) is a potent opioid-like alkaloid associated with kratom, but concentrated 7-OH products are very different from traditional kratom leaf.
- In July 2026, the DEA announced temporary Schedule I control of 7-hydroxymitragynine (7-OH), mitragynine pseudoindoxyl, MGM-15, and MGM-16 while distinguishing qualifying botanical kratom products from synthesized and highly concentrated substances.
- Fatal overdoses and poison center reports linked to concentrated 7-OH products have raised concern among public health agencies, addiction professionals, and regulators.
- 7-OH withdrawal may resemble opioid withdrawal and can include anxiety, insomnia, sweating, nausea, muscle aches, diarrhea, cravings, and mood instability.
- Products containing concentrated 7-OH are widely sold as tablets, gummies, powders, drink shots, and branded alkaloid products, often in gas stations, smoke shops, vape stores, and online marketplaces.
Understanding 7-OH: What Addiction Professionals Need to Know
7-hydroxymitragynine, commonly referred to as 7-OH, is a terpenoid indole alkaloid found in trace amounts in the leaves of Mitragyna speciosa, the tropical tree known as kratom. It may also be produced in the human body as a metabolite of mitragynine, kratom’s primary alkaloid.
The public health concern in 2026 is not ordinary kratom leaf. The concern centers on concentrated, semi-synthetic, and synthetic 7-OH products that expose consumers to much higher levels of opioid-active alkaloids than traditional kratom leaf products.
This distinction is critical for addiction professionals. A client who says “I use kratom” may be referring to whole-leaf powder, kratom capsules, extract shots, concentrated 7-OH tablets, gummies, powders, or semi-synthetic kratom-derived opioid compounds.
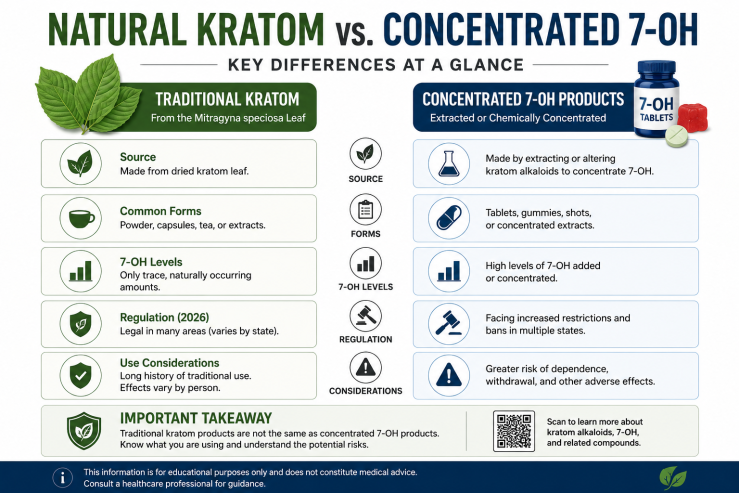
Natural Kratom vs. Concentrated 7-OH
Traditional kratom leaf and concentrated 7-OH products should not be treated as the same exposure. Traditional kratom leaf contains a natural mixture of alkaloids, including mitragynine and only trace amounts of naturally occurring 7-OH. Concentrated 7-OH products may contain elevated levels of opioid-active alkaloids and are commonly sold as tablets, gummies, powders, drink shots, or branded “alkaloid” products.
This distinction matters because concentrated 7-OH products may carry a stronger risk profile for tolerance, dependence, withdrawal, overdose, and regulatory enforcement than traditional kratom leaf.
How Potent Is 7-OH Compared to Morphine and Other Opioids?
As concentrated 7-OH products evolved, researchers and regulators also began monitoring related compounds such as What Is Mitragynine Pseudoindoxyl? The Kratom-Derived Opioid Compound Explained and MGM-16, MGM-15, and 7-OH: Understanding the New Generation of Semi-Synthetic Kratom Opioids. These compounds represent the next generation of semi-synthetic kratom-derived opioid compounds and have become a focus of state and federal regulatory actions.
The potency of 7-hydroxymitragynine is what separates it from traditional kratom and places concentrated 7-OH products into a higher-risk category. Research has described 7-OH as a highly active mu-opioid receptor compound with substantially greater opioid receptor activity than mitragynine.
Animal studies have shown that 7-hydroxymitragynine, but not mitragynine, substituted for morphine self-administration in rats in a dose-dependent manner, suggesting meaningful abuse liability. Researchers have also raised concern that 7-OH exposure may increase opioid-seeking behavior in preclinical models.
Clinically, the concern is not only potency. Concentrated 7-OH products may have rapid onset, short duration, and high reinforcement potential. Users may re-dose frequently, develop tolerance quickly, and experience opioid-like withdrawal when they stop.
How 7-OH Is Sold: The “Gas Station Opioid” Problem
Concentrated 7-OH products are widely available in forms that may look like supplements, candy, or over-the-counter wellness products. These products may be marketed with vague terms such as “plant alkaloids,” “advanced kratom alkaloids,” or “7-hydroxy” without clearly communicating opioid-like risk.
Common product forms include:
- Tablets: Often sold in small packages with milligram-level claims and branding that may not clearly explain opioid-like risk.
- Gummies and candy-like products: Flavored products that may appear less dangerous than pills, powders, or opioid drugs.
- Drink shots and mixes: Liquid products marketed alongside energy shots, supplements, and convenience-store wellness products.
- Powders and capsules: Often sold online with vague labeling such as “alkaloid extract” or “plant alkaloid.”
- Vape or inhaled products: Higher-risk product forms because inhalation may produce faster onset and more compulsive use patterns.
In July 2025, the FDA issued warning letters to companies marketing concentrated 7-OH products as dietary supplements, foods, or unapproved drugs. In 2026, federal and state regulators escalated their response through controlled-substance scheduling actions.
Confirmed Deaths and Rising Emergency Department Visits
The public health data surrounding concentrated 7-OH products has escalated rapidly. Health agencies and poison centers have reported severe illness, respiratory depression, emergency department visits, and fatal overdoses associated with concentrated 7-OH products.
These incidents underscore a critical clinical reality: high doses of 7-OH, especially when combined with alcohol, benzodiazepines, sleep medications, opioids, gabapentin, pregabalin, or other sedating substances, may cause severe respiratory depression and death.
Because 7-OH acts through opioid receptors, naloxone (Narcan) may reverse 7-OH toxicity, although repeated doses may be required. Suspected 7-OH overdose should be treated as a medical emergency. Call 911 immediately.
7-OH Addiction: What the Science Says About Dependence Risk
Multiple lines of evidence point to significant addiction potential for concentrated 7-OH products. Researchers have warned that chronic 7-hydroxymitragynine product use may result in opioid-like physical dependence and addiction.
Clinicians should consider screening patients for both Kratom Use Disorder and Opioid Use Disorder when concentrated 7-OH products are involved. This is especially important when a patient reports daily use, escalating doses, withdrawal symptoms, cravings, unsuccessful attempts to stop, or continued use despite consequences.
Users may describe the effects of 7-OH as euphoric, calming, pain-relieving, anxiety-reducing, or opioid-like. However, the same effects that make these products attractive to consumers may also increase the risk of dependence, compulsive use, withdrawal, and relapse.
7-OH Withdrawal: Duration, Symptoms, and Treatment Challenges
7-OH withdrawal is one of the most clinically significant challenges for addiction treatment professionals encountering this substance. Withdrawal experiences vary, but symptoms may resemble opioid withdrawal.
Common symptoms may include:
- Anxiety or panic
- Restlessness
- Insomnia
- Muscle aches
- Sweating or chills
- Nausea, vomiting, or diarrhea
- Irritability
- Depressed mood
- Cravings
- Restless legs
The withdrawal timeline generally follows three phases:
Acute Phase: Days 1–7
The most severe physical symptoms may include muscle pain, nausea, vomiting, insomnia, anxiety, sweating, agitation, and gastrointestinal distress.
Sub-Acute Phase: Weeks 1–3
Fatigue, mood instability, poor concentration, irritability, cravings, and ongoing sleep disturbance may persist after the most intense physical symptoms improve.
Post-Acute Symptoms: Weeks to Months
Some individuals experience emotional instability, cognitive difficulty, anhedonia, cravings, and sleep disruption for weeks or longer, especially after heavy or prolonged use.
Buprenorphine and buprenorphine-naloxone have been used off-label in some cases involving kratom or 7-OH withdrawal. However, treatment should be individualized and supervised by qualified medical professionals. People should not self-start Suboxone after using 7-OH or kratom products because timing, dependence severity, and precipitated withdrawal risk require clinical evaluation.
For more detail, read 7-OH Withdrawal: Symptoms, Timeline, and Treatment Considerations and Does Suboxone Help Kratom / 7-OH Withdrawal?.
2026 DEA and State Legal Update
The regulatory landscape for 7-OH changed significantly in 2026. In July 2026, the U.S. Drug Enforcement Administration announced temporary Schedule I control of 7-hydroxymitragynine (7-OH), mitragynine pseudoindoxyl, MGM-15, and MGM-16.
The DEA made an important distinction: the temporary scheduling action does not apply to botanical kratom products containing naturally occurring 7-OH below the specified threshold. Instead, the action targets synthesized products and products containing elevated concentrations of 7-OH-related substances.
Florida also acted in June 2026, placing highly concentrated 7-OH and related compounds into Schedule I under state law. Florida’s emergency rule named 7-OH, mitragynine pseudoindoxyl, 7-acetoxymitragynine, MGM-15, MGM-16, and related compounds.
Several states already restrict kratom or kratom-related alkaloids, while others are pursuing age restrictions, labeling rules, product-form restrictions, or bans on synthetic and concentrated 7-OH products. Addiction professionals, clinicians, retailers, and consumers should verify current federal, state, and local law before relying on any legal-status summary.
For a deeper explanation of the related compounds named in recent regulatory actions, see MGM-16, MGM-15, and 7-OH: Understanding the New Generation of Semi-Synthetic Kratom Opioids and What Is Mitragynine Pseudoindoxyl? The Kratom-Derived Opioid Compound Explained.
Clinical Implications for Addiction Treatment Professionals
The emergence of concentrated 7-OH products presents several challenges for treatment providers, intervention professionals, emergency responders, and clinical staff.
Assessment: Clinicians should ask specific questions about product type. “Kratom” may refer to whole-leaf powder, capsules, extracts, drink shots, concentrated 7-OH tablets, gummies, powders, or synthetic and semi-synthetic products. Product name, dose, frequency, route of use, and co-use with alcohol or sedatives should be documented.
Testing: Standard drug panels do not reliably screen for kratom alkaloids or 7-OH. Specialized toxicology testing may be required, and results can be limited by sample timing, product variability, and laboratory methodology.
Treatment Planning: Patients with heavy 7-OH use may require medically supervised detoxification, withdrawal management, medication evaluation, and longer continuing care. Residential treatment, partial hospitalization, intensive outpatient programming, and relapse prevention planning may be appropriate depending on severity.
Overdose Response: Treatment centers, families, and first responders should understand that suspected 7-OH overdose should be treated like an opioid-related emergency. Call 911 and administer naloxone when available.
Navigating Treatment for 7-OH Dependence in New York State
For individuals and families in New York State dealing with 7-OH or kratom dependence, professional guidance is essential. Addiction treatment navigation services can help connect individuals to appropriate levels of care, including medically supervised detox, residential treatment, partial hospitalization, intensive outpatient treatment, and continuing care.
- Addiction treatment navigation in New York’s Capital Region and Hudson Valley — Connects individuals and families with medically supervised detox, residential treatment, outpatient care, and recovery resources serving Albany, Troy, Schenectady, Saratoga Springs, and surrounding communities.
- Hudson Valley addiction treatment resources — Information and treatment navigation for substance use disorders throughout Newburgh, Poughkeepsie, Kingston, Middletown, and the greater Hudson Valley.
- Long Island kratom and addiction treatment resources — Treatment navigation for Long Island and the New York metropolitan area, including resources for kratom dependence, 7-hydroxymitragynine (7-OH), opioid use disorders, and medically supervised detoxification.
- Professional drug and alcohol intervention services in New York — Family intervention planning and treatment placement services throughout New York State for individuals struggling with substance use disorders.
The SAMHSA National Helpline is available 24 hours a day, 7 days a week at 1-800-662-4357 for free, confidential treatment referrals and information.
Conclusion: 7-OH Represents a New Chapter in the Opioid Crisis
The rapid proliferation of concentrated 7-hydroxymitragynine products — from gas station shelves to online retailers — represents one of the most significant emerging substance use challenges facing addiction professionals in 2026. These products are often sold in consumer-friendly forms, marketed through kratom-adjacent language, and purchased by people who may not understand that concentrated 7-OH can behave very differently from traditional kratom leaf.
The DEA’s July 2026 temporary scheduling announcement marks a major regulatory shift. Federal authorities are now treating 7-OH and related substances as serious public safety threats while distinguishing concentrated and synthetic products from botanical kratom products containing naturally occurring 7-OH below the specified threshold.
For clinicians, interventionists, and treatment providers, the key takeaway is clear: when a client reports kratom use, ask follow-up questions. Determine whether the person is using traditional kratom leaf, kratom extracts, concentrated 7-OH tablets or gummies, or synthetic/semi-synthetic alkaloid products. That distinction may change the clinical risk profile, withdrawal plan, overdose education, and level-of-care recommendation.
Related Clinical Resources
Continue exploring the science, clinical management, public health implications, and regulatory developments surrounding concentrated 7-hydroxymitragynine (7-OH), mitragynine pseudoindoxyl (MP), and emerging semi-synthetic kratom-derived opioids.
Foundational Resources
- What Is 7-OH? The Emerging Opioid Threat Addiction Professionals Need to Understand in 2026
- What Is Mitragynine Pseudoindoxyl? The Kratom-Derived Opioid Compound Explained
- MGM-16, MGM-15, and 7-OH: Understanding the New Generation of Semi-Synthetic Kratom Opioids
Withdrawal & Treatment
- 7-OH Withdrawal: Symptoms, Timeline, and Treatment Considerations
- 7-Hydroxymitragynine (7-OH) and Kratom Withdrawal: Clinical Insights and Buprenorphine-Based Management
- Does Suboxone Help Kratom / 7-OH Withdrawal?
- Does Suboxone Help With Kratom Dependence?
Consumer Safety
- Is 7Tabz Safe? FDA Warnings on Concentrated 7-OH
- Buy 7-OH Online? Risks of Concentrated 7-Hydroxymitragynine
Families & Community Resources
- What New York Families Should Know About 7-Hydroxymitragynine (7-OH) and Mitragynine Pseudoindoxyl (MP)
- Kratom Addiction on Long Island: Understanding 7-Hydroxymitragynine (7-OH)
- Kratom Detox on Long Island (Nassau & Suffolk)
Part of the 7-OH Clinical Education Series
This article is part of an ongoing educational series examining concentrated 7-hydroxymitragynine (7-OH), mitragynine pseudoindoxyl, emerging semi-synthetic kratom-derived opioids, withdrawal management, treatment considerations, and evolving regulatory developments affecting clinicians, addiction professionals, policymakers, and families.
References and Sources
- U.S. Drug Enforcement Administration. “DEA to Temporarily Schedule 7-OH and Related Substances to Protect Public Safety.” July 1, 2026.
- U.S. Food and Drug Administration. “FDA Takes Steps to Restrict 7-OH Opioid Products Threatening American Consumers.” FDA Press Release, July 29, 2025. fda.gov
- Florida Office of the Attorney General. “Attorney General James Uthmeier Signs Emergency Rule Immediately Scheduling Dangerous 7-OH and Related Compounds as Schedule I Controlled Substances.” June 22, 2026. myfloridalegal.com
- Smith KE, Boyer EW, Grundmann O, McCurdy CR, et al. “The rise of novel, semi-synthetic 7-hydroxymitragynine products.” Addiction. December 2024. Wiley Online Library
- Johns Hopkins Medicine. “Emerging Use of Kratom in US: Kratom Use Disorder Experts Propose Decision-Making Algorithm for Clinicians.” February 2025. hopkinsmedicine.org
- Hemby SE, McIntosh S, Leon F, Cutler SJ, McCurdy CR. “Abuse liability and therapeutic potential of the Mitragyna speciosa alkaloids mitragynine and 7-hydroxymitragynine.” Addiction Biology. 2019;24:874–885. PubMed
- University of Illinois at Chicago College of Pharmacy. “Buprenorphine and buprenorphine-naloxone for the treatment of kratom withdrawal.” Drug Information Group FAQ, August 2023. uic.edu
About the Author
Benjamin Zohar, NCACIP is a Nationally Certified Advanced Clinical Intervention Professional, ISSUP New York Network Moderator, NAADAC Professional Member, and CCAPP Individual Member. He specializes in intervention planning, addiction treatment navigation, and evidence-based recovery resources throughout New York State.
Benjamin has authored numerous educational publications covering 7-hydroxymitragynine (7-OH), mitragynine pseudoindoxyl, kratom dependence, emerging semi-synthetic opioids, withdrawal management, intervention strategies, and addiction treatment systems. His work focuses on translating emerging scientific research into practical guidance for clinicians, families, and addiction professionals.
Benjamin Zohar’s 7-OH and kratom-related educational work has been cited or referenced in broader public reporting and discussion around concentrated 7-hydroxymitragynine products, including coverage connected to Newsweek, WIRED, the Orange County Register, and public marketplace/product-safety discussions.
Medical Reviewer: Brandon McNally, RN, provides clinical accuracy review for all published content.
Editorial Support: Ezra Zohar, M.S. Ed.
This article is intended for educational and informational purposes for addiction professionals and the general public. It does not constitute medical advice. Individuals concerned about 7-OH use, kratom dependence, or substance use disorders should consult with qualified healthcare professionals or contact the SAMHSA National Helpline at 1-800-662-4357. If someone may be overdosing, call 911 immediately and administer naloxone if available.