Codeine Withdrawal: Symptoms, Timeline & Treatment
The Integrated Recovery & Intervention Education Network (IRIEN) is a professional hub moderated by Benjamin Zohar for sharing evidence-based insights, experiences, and resources across the continuum of addiction care. Back to Integrated Recovery & Intervention Education Network (IRIEN) main page
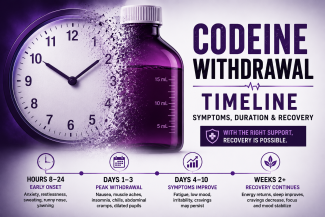
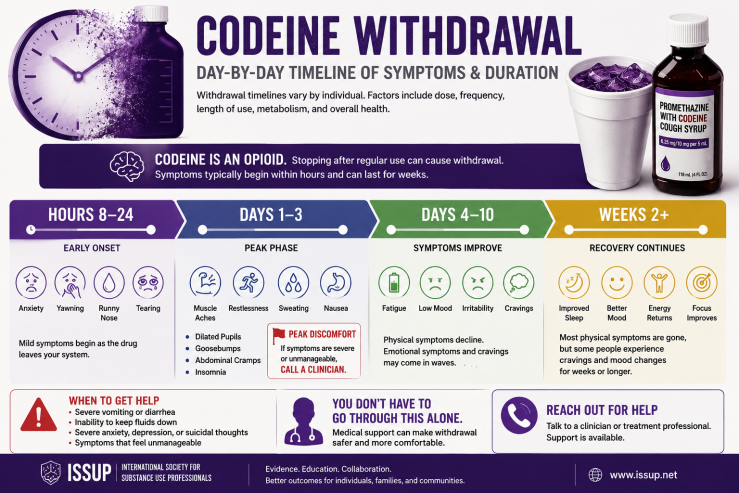
Codeine withdrawal is a classic opioid withdrawal syndrome that develops after regular use stops — whether the codeine came from tablets or from lean (also called "dirty sprite" or "purple drank"). Symptoms include anxiety, muscle aches, sweating, gastrointestinal distress, insomnia, and cravings; they typically begin within 8–24 hours of the last dose, peak around days 1–3, and largely resolve within 4–10 days. Because codeine is an opioid, it is also detected on standard opiate drug tests.
Key Takeaways
- Codeine is a short-acting opioid; withdrawal onset is early — usually within 8–24 hours of the last dose.
- Acute symptoms peak around days 1–3 and mostly resolve by days 4–10; protracted symptoms (insomnia, low mood, cravings) can last weeks.
- Codeine withdrawal is rarely life-threatening — unlike alcohol or benzodiazepine withdrawal — but it is a major relapse driver, which is the real clinical risk.
- People withdrawing from lean/purple drank often also used alcohol or benzodiazepines; co-dependence changes the safety picture and must be assessed before any home-based plan.
- Yes, purple drank shows up on a drug test. Codeine is a standard SAMHSA-5 opiate; urine detects it for roughly 1–3 days (longer with heavy use), and hair for up to 90 days.
- Buprenorphine-based management, structured tapers, and supportive medications are all evidence-based; abrupt unsupported cessation has the worst relapse profile.
Table of Contents
- Why Codeine Causes Withdrawal
- Codeine Withdrawal Symptoms
- Codeine Withdrawal Timeline
- Withdrawal After Lean (Purple Drank) Use
- How Bad Is Codeine Withdrawal?
- Does Purple Drank Show Up on a Drug Test?
- Promethazine and Drug-Test Interpretation
- Treatment Considerations
- When to Seek Help
- Frequently Asked Questions
- Related Clinical Resources
- References
Why Codeine Causes Withdrawal
Codeine is an opioid, and its withdrawal follows standard opioid neuroadaptation: with regular exposure the nervous system downregulates its response to mu-opioid stimulation, and when the drug is removed the system rebounds into overdrive. Codeine's short half-life (roughly three to four hours) means blood levels fall quickly, producing an earlier withdrawal onset than long-acting opioids. Because codeine is a prodrug converted to morphine by the CYP2D6 enzyme, individual metabolizer status also shapes both dependence and withdrawal intensity — ultra-rapid metabolizers sustain higher morphine exposure and may experience stronger withdrawal.
Codeine Withdrawal Symptoms
Codeine withdrawal presents with the recognizable opioid pattern, typically in two waves:
- Early symptoms (first 24 hours): anxiety and restlessness, yawning, runny nose, tearing, sweating, muscle aches, irritability, cravings, disturbed sleep.
- Peak symptoms (days 1–3): nausea, vomiting, diarrhea, abdominal cramping, gooseflesh, chills alternating with sweats, dilated pupils, elevated heart rate and blood pressure, insomnia, intense cravings, low mood.
Symptoms are frequently described as a severe flu combined with agitation and sleeplessness. Dehydration from gastrointestinal losses is the most common complication requiring attention.
Codeine Withdrawal Timeline
| Phase | Typical timing | What happens |
|---|---|---|
| Onset | 8–24 hours after last dose | Anxiety, yawning, sweating, runny nose, muscle aches, cravings begin |
| Peak | Days 1–3 | Gastrointestinal symptoms, chills, insomnia, elevated pulse, strongest cravings |
| Resolution | Days 4–10 | Physical symptoms taper; appetite and energy begin returning |
| Protracted phase | Weeks 2+ | Sleep disturbance, low mood, anhedonia, intermittent cravings in some individuals |
Timing varies with dose, duration of use, metabolism, age, and co-used substances. Heavier and longer use shifts the curve later and longer.
Withdrawal After Lean (Purple Drank) Use
Withdrawal from lean is codeine withdrawal — the promethazine component does not produce a comparable dependence syndrome, though stopping it can unmask rebound insomnia given how sedating the combination was. Three lean-specific considerations matter clinically:
- Unknown dose history. Homemade mixtures make it impossible to estimate daily codeine intake accurately, so withdrawal severity is harder to predict than with tablet-based use.
- Frequent co-use. Lean is commonly consumed with alcohol, cannabis, or benzodiazepines. Alcohol and benzodiazepine dependence change withdrawal management entirely — their withdrawal syndromes can be medically dangerous in ways codeine's is not — so screening for co-dependence is the first step before any cessation plan. The comparative pharmacology in Xanax vs Valium vs Ativan vs Klonopin: Key Differences outlines why benzodiazepine involvement escalates the safety picture.
- Age of the typical user. Lean use concentrates in adolescents and young adults; withdrawal management in minors should involve clinicians experienced with adolescent substance use rather than improvised home detox. For the full substance profile, see the cornerstone guide What Is Lean (Dirty Sprite)? Risks, Slang & Treatment.
How Bad Is Codeine Withdrawal?
On the opioid spectrum, codeine withdrawal is generally milder than withdrawal from heroin, fentanyl, or high-dose oxycodone, reflecting codeine's lower potency. It is rarely dangerous for otherwise healthy adults. Its clinical significance lies elsewhere: the discomfort is more than enough to drive continued use, and unsupported "cold turkey" attempts have high relapse rates. Relapse after even a short abstinent period also lowers tolerance, raising overdose risk on resumption — the standard opioid-relapse hazard. The terminology and clinical meaning of relapse are covered in the IRIEN glossary; see Abstinence — Definition, Meaning in Addiction Recovery, and Why the Term Is Contested.
Does Purple Drank Show Up on a Drug Test?
Yes. Purple drank (lean) contains codeine, which is a standard opiate detected on routine drug tests. Codeine is one of the SAMHSA-5 opiates screened on most urine panels, and it partially metabolizes to morphine, which tests also detect. How long it remains detectable depends on the test type, dose, frequency of use, metabolism, and hydration.
| Test type | General codeine detection window |
|---|---|
| Urine | About 1–3 days for occasional use; up to roughly 4 days, sometimes longer, with heavy or chronic use. Urine is the most common method. |
| Blood | Shortest window — typically only a few hours up to about 24 hours after use. |
| Saliva | Roughly 1–4 days, though results vary considerably between individuals and test devices. |
| Hair | Longest window — up to about 90 days, reflecting historical rather than recent use. |
These are general estimates, not guarantees. Detection windows should never be used to time use or to guide unsafe medication decisions.
Promethazine and Drug-Test Interpretation
Two separate points about lean and drug testing are worth distinguishing, because they are easy to conflate:
- Codeine itself is a true positive, not a false one. On an opiate immunoassay, codeine produces a genuine opiate-positive result. A positive opiate screen after lean use is expected and can be confirmed with a more specific method — gas chromatography–mass spectrometry (GC-MS) or LC-MS/MS — which identifies codeine and morphine specifically rather than "opiates" as a class.
- False positives on rapid screens come from other ingredients and lookalikes, not codeine. Several over-the-counter substances — including diphenhydramine, doxylamine, and dextromethorphan — can trigger false-positive opiate results on some rapid immunoassays; these are common in cough-and-cold products a lean user might also be taking. Any unexpected screening result should be resolved with confirmatory GC-MS testing before conclusions are drawn.
Clinical Pearl: A patient who reports "lean" use but returns a negative opiate screen has not necessarily been dishonest. Counterfeit street "syrup" may contain no codeine at all, substituting other sedatives — so a negative opiate screen in a symptomatic patient should prompt broader toxicology, not dismissal. Conversely, confirm any unexpected positive with GC-MS before acting on it, since rapid immunoassays cross-react with common cough-and-cold ingredients.
Treatment Considerations
Evidence-based options for codeine dependence parallel those for other opioid use disorders, scaled to severity:
- Medical assessment first — quantify use as well as possible, screen for alcohol/benzodiazepine co-dependence, assess mental health and hydration.
- Supervised taper — gradual dose reduction under prescriber guidance, appropriate for lower-severity dependence.
- Buprenorphine-based management — effective for moderate-to-severe codeine dependence; induction timing follows standard short-acting-opioid protocols. Practical dosing questions are addressed in Signs Your Suboxone Dose Is Too Low (Cravings, Withdrawal & What to Do), and the buprenorphine framework applied to another opioid-active substance is detailed in 7-Hydroxymitragynine (7-OH) and Kratom Withdrawal: Clinical Insights and Buprenorphine-Based Management.
- Supportive medications — clinicians may use comfort medications for gastrointestinal symptoms, sleep, and autonomic symptoms during acute withdrawal.
- Continuing care — counseling, family involvement (particularly for adolescent patients), and relapse-prevention structure; withdrawal management alone, without follow-on care, predicts relapse.
When to Seek Help
Professional help is appropriate if someone cannot stop or reduce codeine or lean use, experiences withdrawal between uses, needs escalating amounts, combines codeine with alcohol or benzodiazepines, or is an adolescent using at any level. Severe vomiting, inability to keep fluids down, confusion, or any suggestion of co-occurring alcohol/benzodiazepine withdrawal warrants prompt medical evaluation. A community-level guide to local options is available at Lean on Long Island: Dirty Sprite, Fake Syrup Risks, Withdrawal & Treatment Options, and SAMHSA's National Helpline (1-800-662-4357) provides confidential referral nationwide
For people on Long Island dealing with codeine misuse, opioid dependence, or withdrawal symptoms, codeine addiction treatment on Long Island can help connect families with structured opioid treatment options.
Frequently Asked Questions
Does purple drank show up on a drug test?
Yes. Purple drank contains codeine, a standard opiate detected on routine drug tests. Codeine shows in urine for roughly 1–3 days (longer with heavy use), in blood for up to about 24 hours, in saliva for 1–4 days, and in hair for up to about 90 days.
How long does codeine withdrawal last?
Acute codeine withdrawal typically begins 8–24 hours after the last dose, peaks around days 1–3, and largely resolves within 4–10 days. Sleep problems, low mood, and cravings can persist for weeks after heavy or prolonged use.
Can codeine withdrawal kill you?
Codeine withdrawal is rarely life-threatening in otherwise healthy adults, unlike alcohol or benzodiazepine withdrawal. The main risks are dehydration from vomiting and diarrhea — and relapse with lowered tolerance, which raises overdose risk.
Does lean cause a false positive for anything?
Codeine itself produces a true opiate positive, not a false one. However, other cough-and-cold ingredients a lean user might take — such as diphenhydramine, doxylamine, or dextromethorphan — can trigger false-positive opiate results on some rapid screens. Confirmatory GC-MS testing resolves the ambiguity.
Can you quit lean cold turkey?
Physically, most healthy adults can — but unsupported abrupt cessation has the highest relapse rate, and any alcohol or benzodiazepine co-dependence makes it unsafe. A medical assessment first, then a taper or buprenorphine-based plan, produces better outcomes.
Does Suboxone work for codeine dependence?
Buprenorphine-based treatment is effective for codeine dependence, following standard short-acting-opioid induction protocols. Whether it is indicated depends on severity; a prescriber experienced in opioid use disorder should make that determination.
Related Clinical Resources
- What Is Lean (Dirty Sprite)? Risks, Slang & Treatment — a full guide to what lean is, its risks, slang, and treatment options.
- 7-OH Withdrawal: Symptoms, Timeline, and Treatment Considerations — what withdrawal looks like from 7-OH, another opioid-active substance.
- 7-Hydroxymitragynine (7-OH) and Kratom Withdrawal: Clinical Insights and Buprenorphine-Based Management — buprenorphine management detail.
- Signs Your Suboxone Dose Is Too Low (Cravings, Withdrawal & What to Do) — practical MAT dosing questions.
- Does Suboxone Help With Kratom Dependence? — family-facing MAT overview.
- Abstinence — Definition, Meaning in Addiction Recovery, and Why the Term Is Contested — what abstinence and relapse mean in recovery, and why the terms are debated.
Last updated: July 5, 2026
References
- MedlinePlus (U.S. National Library of Medicine). "Opioid Testing." (Opiates include codeine and morphine; urine is the primary matrix.) https://medlineplus.gov/lab-tests/opioid-testing/
- Hadland SE, Levy S. "Objective Testing — Urine and Other Drug Tests." Child Adolesc Psychiatr Clin N Am, 2016. PMC4920965. (SAMHSA-5 opiate panel; detection-window principles.) https://pmc.ncbi.nlm.nih.gov/articles/PMC4920965/
- U.S. Food and Drug Administration (FDA). Promethazine Hydrochloride and Codeine Phosphate Oral Solution — Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/008306s033lbl.pdf
- U.S. Drug Enforcement Administration (DEA). "Controlled Substance Schedules." https://www.deadiversion.usdoj.gov/schedules/schedules.html
- Substance Abuse and Mental Health Services Administration (SAMHSA). TIP 63: Medications for Opioid Use Disorder. https://store.samhsa.gov
- "Codeine and promethazine: Exploratory study on 'lean' or 'sizzurp' using national survey data and an online forum." PLOS ONE, 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC10962845/
About the author: Benjamin Zohar is a Nationally Certified Advanced Clinical Intervention Professional (NCACIP), the ISSUP New York Network Moderator, a NAADAC Professional Member, and a CCAPP Individual Member. He has worked in addiction treatment navigation, crisis intervention, and recovery support for over a decade across New York State
Medical review: Brandon McNally, RN — Registered Nurse specializing in addiction medicine.
This article is for educational and informational purposes only and does not constitute medical advice or a diagnosis. If someone may be overdosing, call 911 immediately and administer naloxone if available. If you or a loved one may be struggling with substance use, consult a qualified professional.